Virtual Reality Relaxation to Decrease Dental Anxiety: Immediate Effect Randomized Clinical Trial
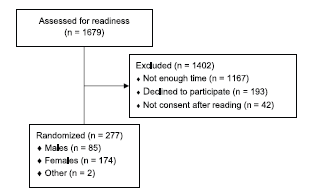
ABSTRACT Introduction: Dental anxiety is common and causes symptomatic use of oral health services. Objectives: The aim was to study […]

ABSTRACT Introduction: Dental anxiety is common and causes symptomatic use of oral health services. Objectives: The aim was to study […]
ABSTRACT Untreated dental decay is the most prevalent dental problem in the world, affecting up to 2.4 billion people and
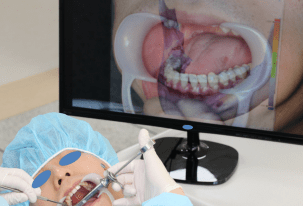
ABSTRACT Efforts to apply augmented reality (AR) technology in the medical field include the introduction of AR techniques into dental
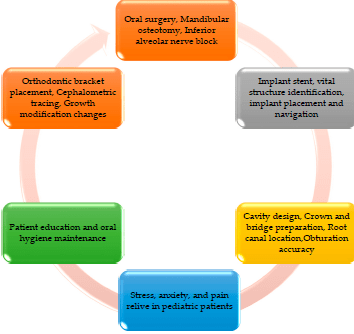
ABSTRACT Abstract: Many modern advancements have taken place in dentistry that have exponentially impacted the progress and practice of dentistry.

ABSTRACT During dental education, dental students learn how to examine patients, make diagnosis, plan treatment and perform dental procedures perfectly

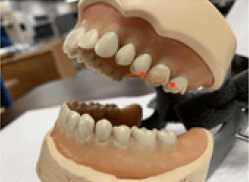
ABSTRACT Summary Statement: In preclinical dental education, the acquisition of clinical, technical skills, and the transfer of these skills to
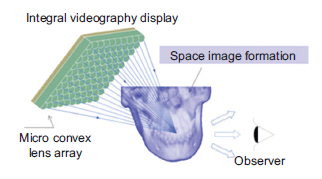
ABSTRACT To evaluate the feasibility and accuracy of a three-dimensional augmented reality system incorporating integral videography for imaging oral and

ABSTRACT Prosthetic dentistry is one of the dental branches that has evolved remarkably, taking advantage of the latest digital innovations.

ABSTRACT Abstract. We present image-based methods for tracking teeth in a video image with respect to a CT scan of

ABSTRACT Background Despite the limited number of articles dedicated to its use, augmented reality (AR) is an emerging technology that