


ABSTRACT
Summary Statement: In preclinical dental education, the acquisition of clinical, technical skills, and the transfer of these skills to the clinic are paramount. Phantom heads provide an efficient way to teach preclinical students dental procedures safely while increasing their dexterity skills considerably. Modern computerized phantom head training units incorporate features of virtual reality technology and the ability to offer concurrent augmented feedback. The aims of this review were to examine and evaluate the dental literature for evidence supporting their use and to discuss the role of augmented feedback versus the facilitator’s instruction. Adjunctive training in these units seems to enhance student’s learning and skill acquisition and reduce the required faculty supervision time. However, the virtual augmented feedback cannot be used as the sole method of feedback, and the facilitator’s input is still critical. Well-powered longitudinal randomized trials exploring the impact of these units on student’s clinical performance and issues of cost-effectiveness are warranted.
(Sim Healthcare 12:332–338, 2017)
Key Words: Dental education, faculty, simulation training
INTRODUCTION
Operative dentistry is a demanding area of clinical education. The development of clinical competence requires the assimilation of large amounts of knowledge combined with the acquisition of clinical skills and problem-solving ability. One of the most essential clinical skills in operative dentistry is preparing and restoring carious teeth. The student needs to comprehend the concepts of the procedure and develop the fine motor skills to perform it. The acquisition of clinical, technical skills, and the transfer of these skills to the clinic, where real patients are treated, is of paramount importance. This can be achieved by vigorous training on phantom heads. Phantom heads provide an efficient way to teach preclinical students dental procedures safely while increasing their psychomotor skills considerably.
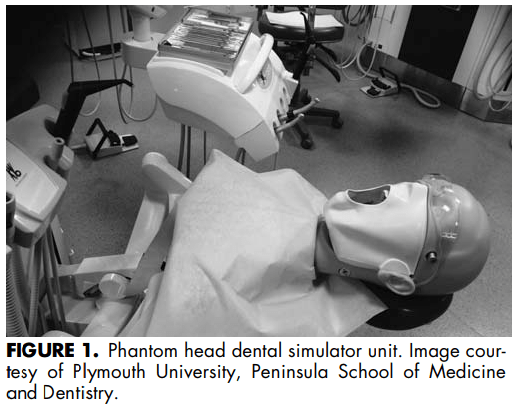
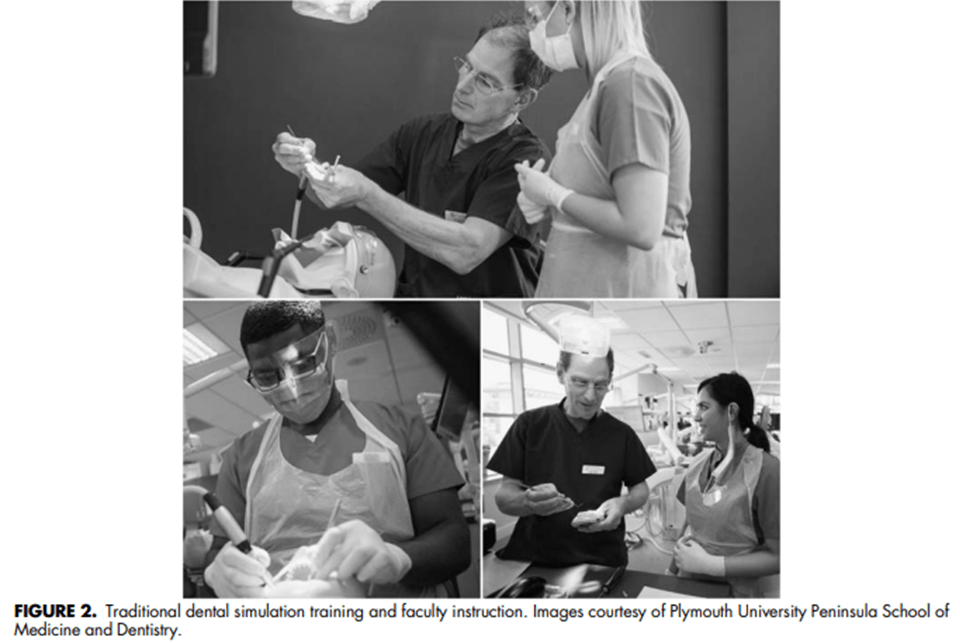
Phantom heads have been the cornerstone of learning in operative dentistry worldwide since their introduction in 1894. The phantom head is affixed to a dental operating unit with a torso, in a manner that allows adjustment of position to allow the students to work in a seated position as they would in a clinical setting. The heads also have a rubber sheet, which provides an approximation of the patient’s cheeks and mouth opening (Fig. 1). Phantom heads replicate the real-life clinical environment including positioning of the operator and the patient, performing dental procedures with an assistant, and infection control procedures.3 Traditionally in preclinical simulation training, the students are shown models, diagrams, and pictures and are asked to repeatedly perform dental procedures on plastic phantom head teeth.[6]The learners receive verbal feedback by a faculty instructor when they have completed all or a portion of a cavity or tooth preparation task (Fig. 2).
In recent years, technological advances have facilitated the incorporation of virtual reality simulation technology in preclinical operative dental education. Virtual reality simulators provide the opportunity for integrating clinical case scenarios in the operative teaching environment and also facilitating the tactile diagnostic skills by utilizing haptic technology. To date, two types of computerized virtual reality dental simulators are available: mannequin-based simulators on which certain dental procedures can be performed using real dental instruments (eg, DentSim TM and Image Guided Implantology IGI both produced by the DenX, Ltd) and haptic-based simulators, which employ a haptic device and virtual models of a human tooth or mouth as a platform for facilitating the practice of dental procedures (eg, PHANToM TM, Virtual Reality Dental Training System VRDTS, Iowa Dental Surgical Simulator, HapTEL, VirDenT & Moog Simodont Dental Trainer).
The mannequin-based computerized simulators combine the benefits of training on a traditional phantom head operating unit, with the benefits of virtual reality simulation.These computerized virtual reality simulators (CVRS) were the focus of this review.
A computerized phantom head dental simulator, which incorporates virtual reality features and provides augmented visual feedback, is the DentSim unit. It has been available since 1997 and has been used and evaluated in Dental Institutions in the United States, Europe, and Asia. The unit includes a phantom head, a dental hand piece, a light source, an infrared camera, and two computers.
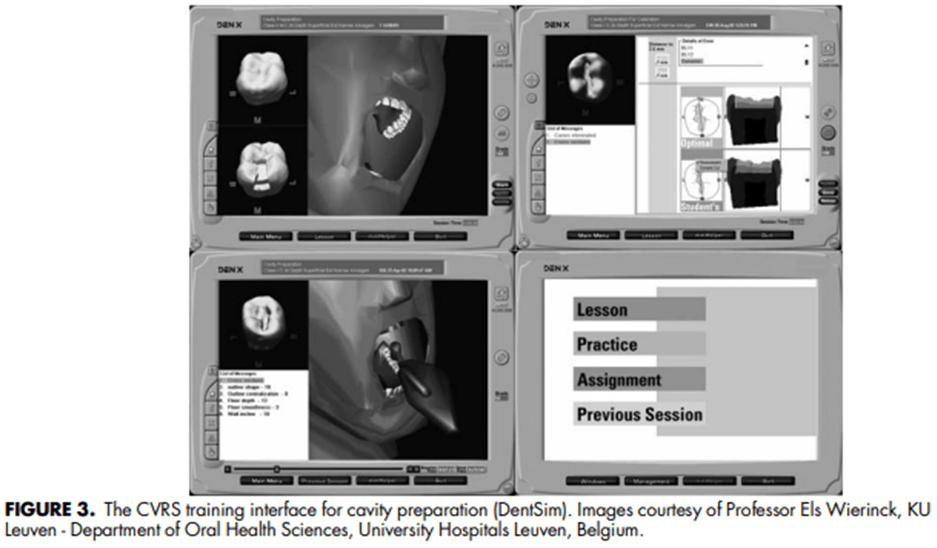
The phantom head and handpiece contain infrared emitters that allow the infrared camera to detect their spatial orientation in space. As a student prepares a cavity in the phantom head, the software formulates a virtual three-dimensional representation of the preparation in progress, which is presented on the computer screen (Fig. 3). The student’s cavity preparation can be compared with the ideal cavity preparation by overlaying the two virtual reality images at any time during the procedure. Procedural errors are audio signaled as they are made and the generated error messages can be viewed immediately.
A final evaluation report and a list of errors become available at the end of the procedure.6,12 The virtual environment is enhanced with complete patient records including examination notes and radiographs, which provide a more realistic environment, bringing the technical tasks into a clinical context, during the simulation training.12 The aim of this review was to examine and evaluate the existing body of literature on the use of the CVRS in preclinical dental education. The impact on student’s performance and learning experience, as well as the role of the faculty instruction versus the augmented visual feedback provided by these units, in the clinical skills acquisition simulation training, is discussed.
METHODS
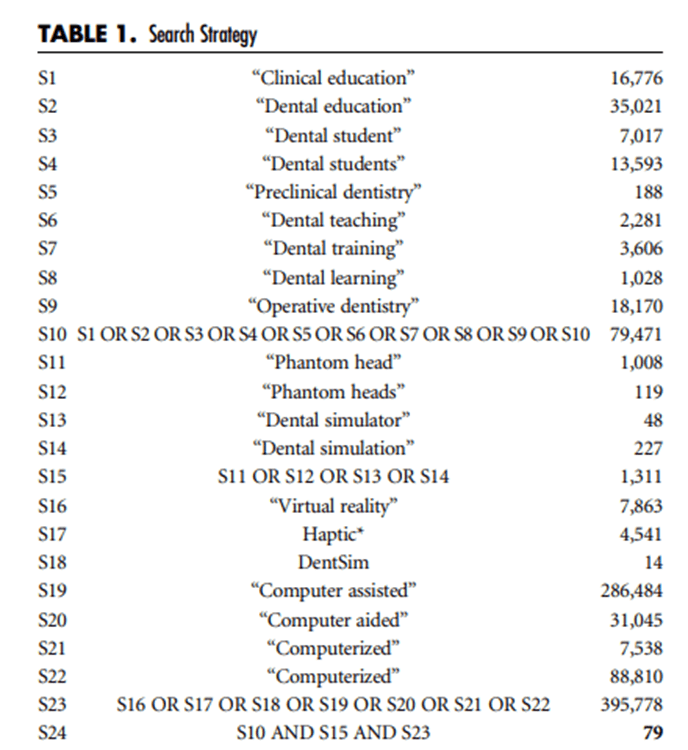
A search of the literature was performed searching the following databases via EBSCO: Medline, British Educational Index, and ERIC. The search terms used and the search strategy can be found in Table 1. Articles in which the CVRS were discussed in terms of preclinical dental education were included. Studies using CVRS in postgraduate dental education as well studies using haptic technology simulation systems were excluded. Only studies in the English language were considered for inclusion. Finally, no limits for study design were applied.
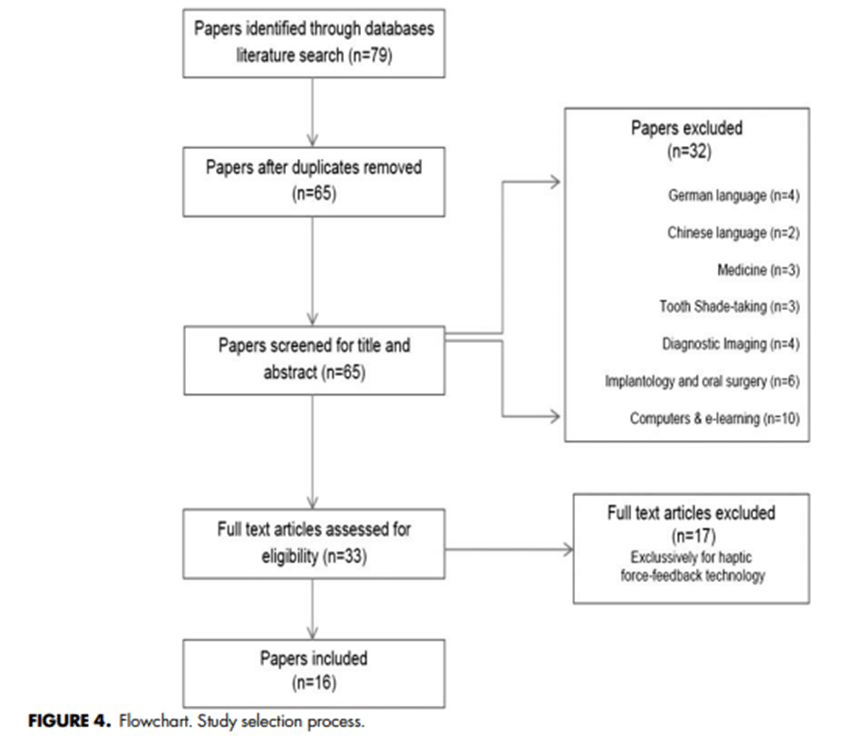
The citations retrieved from the above search (79) were inserted into the reference management software Endnote X7.4. The titles and abstracts were screened for relevance. The potentially relevant papers (33) were accessed and read in full text. The selection process of the included studies (16) and the reasons for exclusion are depicted in the PRISMA flowchart (Fig. 4).
RESULTS
Impact on Student Performance
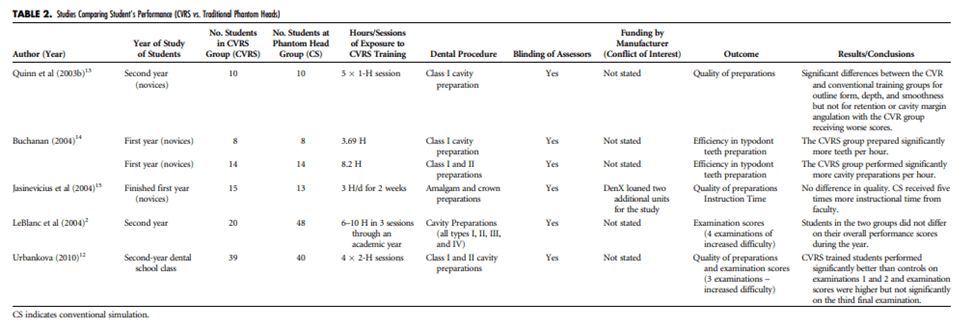
From the 79 articles retrieved, 16 were deemed relevant and were included in this review. From these, five prospective experimental studies assessed the students’ performance in cavity preparation after additional training on the CVRS. The main characteristics and results of these studies can be found in Table2. Concerning the quality of tooth preparations, most of the studies found no significant differences between those who trained solely on conventional phantom heads versus those who had been exposed adjunctively to the CVRS.
Conversely, Kikuchi et al demonstrated that students using the CVRS units performed better quality crown preparations than those who did not. Similarly, when first-year dental students received 8 hours of adjunctive computerized dental simulation training, although they performed better early in the study, their clinical performance did not differ as assessed by the final practical examination. As the retention and transferability of skill and knowledge are concerned, several studies found no significant differences in the final practical examination scores. LeBlanc et al did not identify any marked differences in the final examination scores but observed a more significant improvement between the first and final assessment scores for the CVRS group. In contrast, Maggio et al18, suggested that the introduction of the CVRS in preclinical dental training resulted in a reduction in the course remediation rate and reduction of the course failure rates by more than a half.
Time Efficiency
In an experimental study at the University of Pennsylvania, the students who received CVRS training showed a higher efficiency in cavity preparations than the students who trained on the traditional phantom heads. Namely, they prepared significantly more teeth per hour (3.8 vs. 1.6) and used more teeth (average of 11.71 vs. 6.57 for control, P = 0.02) during their practising session.[14] Similarly, training sessions with CVRS shortened the crown preparation time performed by fifth-year dental students at Tokyo Medical and Dental University.[9] Besides, virtual reality simulators seem to reduce the required instruction and supervision time by faculty members of staff.[14] Jasinevicius et al [15] demonstrated that students who were trained on conventional simulators received five times more instructional time from faculty than students who were trained on virtual reality ones. However, there were no statistically significant differences in the quality of the preparations despite the additional instructional time.
Student Learning Experience
Several studies have surveyed dental students about their preferences over conventional or virtual reality simulation. The CVRS training seems to be rated rather positively by the students. Most (87.3%) of first-year students at Tennessee Dental school working with CVRS found the experience to be “very interesting” or “interesting.” [11] Among the positive features of virtual reality simulators, as perceived by dental students, were the positive impact on improving their manual and motor skills, the increased speed and number of preparations,the access to feedback,the ability for the student to monitor their own work without involvement of a supervisor, the preparation for assessment, the consistency of evaluation, and the allowance for self-paced learning. Students criticized the CVRS for excessive feedback, lack of personal contact, and technical difficulties with hardware.[13,16] In addition, students agreed that virtual reality simulators could not fully replace the conventional phantom heads, and the combination of the two is the most preferable and effective way of learning.[13,16] On the other hand, students found that the feedback and supervision by faculty facilitators can be inconsistent, and supervisors can be too busy, but it increases their confidence in cavity preparations.
Feedback
As far as quality and effectiveness of instruction and feedback is concerned, several studies have suggested that the virtual reality simulator could not be accepted as the sole form of feedback and evaluation the students should be exposed to. Namely, Urbankova [12] concluded that CVRS-augmented feedback cannot replace human instruction. Quin et al suggested that CVRS is not appropriate as a sole method of feedback and evaluation for novice dental students. This statement agrees with a later study in which sole CVRS feedback was not found beneficial, as the retention and transfer test scores between students who used CVRS versus conventional phantom heads did not differ significantly. By the same token, Wierinck et all have suggested that alternating virtual reality with human instruction and feedback can result in positive learning outcomes.
DISCUSSION
The role of simulation has been recognized as an important aspect of training in healthcare, which supports and improves patient safety. Technology-enhanced simulation, including virtual reality training, has been associated with positive outcomes for healthcare trainee’s knowledge and skills.
The use of virtual reality simulators for the training of novice surgical trainees has been supported by a number of systematic reviews. In laparoscopic surgery, it has been shown to result in a significant reduction in operating time and procedural errors while improving the trainees’ performance scores. Besides, two recent systematic reviews by the Cochrane Collaboration, in the fields of endoscopy and ear, nose, and throat surgery, suggested that virtual reality simulation can be used to supplement traditional surgical training for medical students and surgical trainees with little or no surgical experience.[25,26] Nonetheless, the authors concluded that virtual reality training allows trainees to develop technical skills at least as good as those achieved through conventional training.[25]
Similarly, adjunctive training on the dental CVRS has the potential to improve student’s clinical performance and enhance their practical examination scores.[9,12,13,17] The augmented feedback through visual cues can facilitate proper eye-hand coordination and reduce the number of procedural errors.[12] Confronting the students with their own errors as they are made allows them to visually inspect their work compared with an ideal model [16,17] and instantaneously rectify it, which can potentially increase learning efficiency and skill development.[12] Noteworthily, although students seemed to perform better early after the CVRS training, their clinical performance in final examinations did not differ from that of the students who trained solely on traditional phantomhead units.[12,14,17] The fact that the amount of transfer from one task onto another depends on the similarity of the neural processing demands, underlying motor execution, may offer an explanation.[17] Besides, the transferability of skills from one context to another is not an uncommon finding in healthcare simulation. Namely, studies in the fields of bronchoscopy, endoscopy, and laparoscopic surgery have shown that skills acquired using virtual-reality simulation will transfer to the operating room. [27–29]
Nonetheless, with the expansion of the dental curricular content, the effective use of student’s time has become an increasing necessity. [16] The CVRS training has shown to improve students’ efficiency in teeth preparations [9,14] and reduce the required time for faculty instruction and supervision.[15] Hence, the faculty instructors’ time can be used in teaching the students crucial nonprocedural skills such as patient management, ethics, and teamwork. Sharing their expertise and experiences in the transition of a student from novice to clinician remains critical. [7,12]
The unsuitability of the use of CVRS feedback as the sole method of feedback and evaluation for novice students is a consistent criticism among the included studies.[7,13,16,17] Although CVRS seem to be a reliable method for monitoring technical progress, addressing the issue of lack of reproducibility among assessors[13]; they cannot be used as a substitute for expert feedback. It has been suggested that the extensively detailed and sometimes complex computer feedback can be discouraging and overwhelming, especially for the inexperienced students.[15,17] Appropriate faculty input will reinforce learned theoretical concepts and will provide the students with insight into the weaknesses of their performance.[2,16] Contextual learning will enable the students to achieve a deeper understanding of theoretical concepts and the impact of any procedural errors (eg, the biological, clinical, and medicolegal implications of damaging an adjacent tooth or unnecessarily preparing a rather deep cavity).
In a modern preclinical environment, students will reflect on the feedback received by the simulator, the facilitator, or both. The CVRS can provide the student with continuous (100%) augmented feedback or they can be set to provide feedback less frequently or none at all. In traditional phantom head preclinical courses, the supervisors offer feedback at the end of critical parts of the procedure and the end of the task. Usually, the ratio of supervisors to students does not permit every student to receive constant feedback and instruction during the dental procedure. According to Wierinck et al,
[7] continuous (100%) CVRS feedback during the task did not offer any additional benefit over intermittent (66% of the time) feedback. Nonetheless, a recent meta-analysis suggested that terminal feedback seems more effective than concurrent feedback for novice learners’ skill retention.[30] The mechanism by which feedback may be operating is in line with the guidance hypothesis[31] and, to some extent, the cognitive load theory.[32]
The guidance hypothesis suggests that constant feedback from an instructor during each practice attempt (concurrent feedback) may lead to an overreliance on the feedback such that when feedback is withdrawn, the learner’s performance declines.[30,31] Reduced frequency of instruction may, therefore, enhance motor skill learning and detection of errors.[33] According to the cognitive load theory, feedback provided during a procedural skills session could influence cognitive load, either increasing it by providing “information overload” or decreasing it by structuring the task so that it is better understood.[30,32] Thus, it is plausible that continuous feedback may cognitively overload the learner and hinder their learning.[30]
The included studies assessed the suitability and effectiveness of the CVRS units as an adjunctive training tool for novice dental students. These units can also act as a valid and reliable screening device to capture expert performance. [8] Wierinck et al [8] suggested that the DentSim unit can distinguish different levels of excellence in performance (expert vs. novice). On that ground, CVRS may be used in other areas such as continuing dental education, continued competency of practitioners, clinical board examinations, and remediation of impaired practitioners. [6] Future research will be needed to explore the feasibility of CVRS in these areas. Furthermore, evidence for the long-term effect of CVRS training on the students’ clinical performance and competence as well as data regarding the cost-effectiveness of these devices is currently lacking. Future studies should conform to the extended CONSORT and STROBE reporting guidelines for healthcare simulation research,[20] to ensure complete reporting and transparency in the research conduct.[20,34]
CONCLUSION
The existing body of evidence suggests that combining and alternating the traditional and pioneering simulation methods and feedback may be of benefit to the learners. However, there is insufficient evidence to advise for or against the use of computerized virtual reality simulators as a replacement of the traditional phantom heads and human instruction. Virtual reality simulation may enable a better understanding among learners in a more diverse learning environment and augment rather than replace existing teaching methods that work well such as faculty instruction and feedback. Incorporating such a technology in the dental curriculum can add a substantial expense nevertheless to a dental faculty’s budget. Well-designed and adequately powered long-term prospective studies exploring matters of student performance, learning outcomes, and cost-effectiveness are warranted.
ACKNOWLEDGMENTS
The author thanks the reviewers for their thoughtful comments that substantially improved the quality of this review. In addition, the author thanks Mr. Lloyd Russell (Digital marketing, Plymouth University, England, UK) for kindly offering the images appearing in Figures 1 and 2 and Professor Els Wierinck (KU Leuven – Department of Oral Health Sciences, University Hospitals Leuven, Belgium) for offering the DentSim images appearing in Figure 3. The author is a National Institute for Health Research–funded Academic Clinical Fellow at Peninsula Dental School (Plymouth University).
Source
https://pubmed.ncbi.nlm.nih.gov/28697057/
References
- Duta MA, Bogdan CM, Popovici DM, Ionescu N, Nuca CI. An overview of virtual and augmented reality in dental education. Oral Health Dent Manag 2011;10:42–49.
- LeBlanc VR, Urbankova A, Hadavi F, Lichtenthal RM. A preliminary study in using virtual reality to train dental students. J Dent Educ 2004;68:378–383.
- Suvinen TI, Messer LB, Franco E. Clinical simulation in teaching preclinical dentistry. Eur J Dent Educ 1998;2:25–32.
- Fugill M. Defining the purpose of phantom head. Eur J Dent Educ 2013;17: e1–e4.
- Kapoor S, Arora P, Kapoor V, Jayachandran M, Tiwari M. Haptics -touchfeedback technology widening the horizon of medicine. J Clin Diagn Res 2014;8:294–299.
- Buchanan JA. Use of simulation technology in dental education. J Dent Educ 2001;65:1225–1231.
- Wierinck E, Puttemans V, van Steenberghe D. Effect of reducing frequency of augmented feedback on manual dexterity training and its retention. J Dent 2006;34:641–647.
- Wierinck ER, Puttemans V, Swinnen SP, van Steenberghe D. Expert performance on a virtual reality simulation system. J Dent Educ 2007;71:759–766.
- Kikuchi H, Ikeda M, Araki K. Evaluation of a virtual reality simulation system for porcelain fused to metal crown preparation at Tokyo Medical and Dental University. J Dent Educ 2013;77:782–792.
- Rees JS, Jenkins SM, James T, et al. An initial evaluation of virtual reality simulation in teaching pre-clinical operative dentistry in a UK setting. Eur J Prosthodont Restor Dent 2007;15:89–92.
- Welk A, Maggio MP, Simon JF, et al. Computer-assisted learning and simulation lab with 40 DentSim units. Int J Comput Dent 2008;11:17–40.
- Urbankova A. Impact of computerized dental simulation training on preclinical operative dentistry examination scores. J Dent Educ 2010;74:402–409.
- Quinn F, Keogh P, McDonald A, Hussey D. A pilot study comparing the effectiveness of conventional training and virtual reality simulation in the skills acquisition of junior dental students. Eur J Dent Educ 2003;7:13–19.
- Buchanan JA. Experience with virtual reality-based technology in teaching restorative dental procedures. J Dent Educ 2004;68:1258–1265.
- Jasinevicius TR, Landers M, Nelson S, Urbankova A. An evaluation of two dental simulation systems: virtual reality versus contemporary non-computer-assisted. J Dent Educ 2004;68:1151–1162.
- Quinn F, Keogh P, McDonald A, Hussey D. A study comparing the effectiveness of conventional training and virtual reality simulation in the skills acquisition of junior dental students. Eur J Dent Educ 2003;7:164–169.
- Wierinck E, Puttemans V, Swinnen S, van Steenberghe D. Effect of augmented visual feedback from a virtual reality simulation system on manual dexterity training. Eur J Dent Educ 2005;9:10–16.
- Maggio MP, Berthold P, Gottlieb R. Curriculum changes in preclinical laboratory education with virtual reality-based technology training. J Dent Educ 2005;69:160.
- Maggio MP, Berthold P, Gottlieb R. Virtual Reality-Based Technology (VRBT) training positively enhances performance on preclinical practical examinations. J Dent Educ 2005;69:161.
- Cheng A, Kessler D, Mackinnon R, et al. Reporting guidelines for health care simulation research: extensions to the CONSORT and STROBE statements. Simul Healthc 2016;11:238–248.
- Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA 2011;306:978–988.
- Larsen CR, Oestergaard J, Ottesen BS, Soerensen JL. The efficacy of virtual reality simulation training in laparoscopy: a systematic review of randomized trials. Acta Obstet Gynecol Scand 2012;91:1015–1028.
- Gurusamy K, Aggarwal R, Palanivelu L, Davidson BR. Systematic review of randomized controlled trials on the effectiveness of virtual reality training for laparoscopic surgery. Br J Surg 2008;95:1088–1097.
- Ikonen TS, Antikainen T, Silvennoinen M, Isojärvi J, Mäkinen E, Scheinin TM. Virtual reality simulator training of laparoscopic cholecystectomies – a systematic review. Scand J Surg 2012;101:5–12.
- Piromchai P, Avery A, Laopaiboon M, Kennedy G, O’Leary S. Virtual reality training for improving the skills needed for performing surgery of the ear, nose or throat. Cochrane Database Syst Rev 2015:CD010198.
- Walsh CM, Sherlock ME, Ling SC, Carnahan H. Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy. Cochrane Database Syst Rev 2012:CD008237.
- Palter VN, Grantcharov TP. Virtual reality in surgical skills training. Surg Clin North Am 2010;90:605–617.
- Dawe SR, Windsor JA, Broeders JA, Cregan PC, Hewett PJ, Maddern GJ. A systematic review of surgical skills transfer after simulation-based training: laparoscopic cholecystectomy and endoscopy. Ann Surg 2014;259:236–248.
- Kennedy CC, Maldonado F, Cook DA. Simulation-based bronchoscopy training: systematic review and meta-analysis. Chest 2013;144:183–192.
- Hatala R, Cook DA, Zendejas B, Hamstra SJ, Brydges R. Feedback for simulation-based procedural skills training: a meta-analysis and critical narrative synthesis. Adv Health Sci Educ Theory Pract 2014;19:251–272.
- Salmoni AW, Schmidt RA, Walter CB. Knowledge of results and motor learning: a review and critical reappraisal. Psychol Bull 1984;95:355–386.
- Van Merriënboer JJ, Sweller J. Cognitive load theory and complex learning: recent developments and future directions. Educ Psychol Rev 2005;17:147–177.
- Winstein CJ, Schmidt RA. Reduced frequency of knowledge of results enhances motor skill learning. J Exp Psychol Learn Mem Cogn 1990;16: 677–691.
- Sevdalis N, Nestel D, Kardong-Edgren S, Gaba DM. A joint leap into a future of high-quality simulation research-standardizing the reporting of simulation science. Simul Healthc 2016;11:236–237.