

ABSTRACT
Introduction: Dental anxiety is common and causes symptomatic use of oral health services.
Objectives:
The aim was to study if a short-term virtual reality intervention reduced preoperative dental anxiety.
Methods:
A randomized controlled single-center trial was conducted with 2 parallel arms in a public oral health care unit: virtual reality relaxation (VRR) and treatment as usual (TAU).
The VRR group received a 1- to 3.5-min 360° immersion video of a peaceful virtual landscape with audio features and sound supporting the experience. TAU groups remained seated for 3 min. Of the powered sample of 280 participants, 255 consented and had complete data. Total and secondary sex-specific mixed effects linear regression models were completed for posttest dental anxiety (Modified Dental Anxiety Scale [MDAS] total score) and its 2 factors (anticipatory and treatment-related dental anxiety) adjusted for baseline (pretest) MDAS total and factor scores and age, taking
into account the effect of blocking.
Results:
Total and anticipatory dental anxiety decreased more in the VRR group than the TAU group (β = −0.75, P < .001, for MDAS total score; β = −0.43, P < .001, for anticipatory anxiety score) in patients of a primary dental care clinic. In women, dental anxiety decreased more in VRR than TAU for total MDAS score (β = −1.08, P < .001) and treatment-related dental anxiety (β = −0.597, P = .011). Anticipatory dental anxiety decreased more in VRR than TAU in both men (β = −0.217, P < .026) and women (β = −0.498, P < .001).
Conclusion:
Short application of VRR is both feasible and effective to reduce preoperative dental anxiety in public dental care settings (ClinicalTrials.gov NCT03993080).
Knowledge Transfer Statement:
Dental anxiety, which is a common problem, can be reduced with short application of virtual reality relaxation applied preoperatively in the waiting room. Findings of this study indicate that it is a feasible and effective procedure to help patients with dental anxiety in normal public dental care settings.
Keywords
dental fear, clinical studies/trials, relaxation technics, virtual reality immersion, dental care, public sector
INTRODUCTION
One-third of Finnish adults are anxious of dental treatment to some degree, women more often than men. A tenth are very anxious. The prevalence of dental anxiety has remained stable over the past 10 y (Lahti et al. 2007; Liinavuori et al. 2016). These statistics are similar in other countries (Hägglin et al. 1999; Maggirias and Locker 2002; Thomson et al. 2009; Armfield 2010; Hill et al. 2013; Carlsson et al. 2015). People with extreme dental anxiety are more likely to avoid or delay treatment (Pohjola et al. 2007; Thomson et al. 2010; Åstrøm et al. 2011; Hakeberg and Wide Boman 2017; Liinavuori et al. 2019), Finnish men more often than women (Liinavuori et al. 2019).
Dental anxiety may be managed by psychotherapeutic interventions, which enable patients to feel more comfortable when receiving the treatment and which help those patients not visiting the dentist due to a high fear to attend the treatment. These interventions include relaxation, distraction, exposure, and other forms of cognitive behavioral therapy (Armfield and Heaton 2013; Gordon et al. 2013; Wide Boman et al. 2013; Craske et al. 2014). Of these, relaxation and distraction are mostly used during dental treatment, whereas exposure therapy, including inhibitory learning, and other forms of cognitive behavioral therapy might be needed before the dental treatment (Armfield and Heaton 2013; Craske et al. 2014). While some of these interventions may be conducted by a dentist, others require support from psychologists (Armfield and Heaton 2013; Wide Boman et al. 2013). Several treatment visits are usually needed to manage dental anxiety, especially for those with extreme dental anxiety; however, a single appointment to reduce dental anxiety has also shown some success (Armfield and Heaton 2013; Gordon et al. 2013; Wide Boman et al. 2013). Based on this research evidence, a brief patient-centered intervention is needed that may be routinely incorporated into daily practice in primary dental care. New technologies have been developed, such as computer-assisted cognitive behavioral therapy, which has shown some potential (Rooksby et al. 2015; Tellez et al. 2015). Technologies based on virtual reality have also been developed for managing dental anxiety. A systematic review concluded that they have potential, though more rigorous studies are needed (Gujjar et al. 2019a). Many of them are based on distraction during normal or simulated treatment or exposure before treatment and used, for example, natural scenery, games, or information on treatment (Frere et al. 2001; Asl Aminabadi et al. 2012; Tanja-Dijkstra et al. 2014; Kazancioglu et al. 2015; Padrino-Barrios et al. 2015; Atzori et al. 2018; Niharika et al. 2018; Shetty et al. 2019), while others are based on psychologist-delivered cognitive behavioral therapy (Raghav et al. 2016; Gujjar et al. 2017; Gujjar et al. 2019b). Short virtual reality–based interventions have shown particular promise in reducing preoperative or anticipatory anxiety in secondary care (Ganry et al. 2018). We are unaware, however, of short virtual reality–based relaxation being applied in primary dental care preoperatively.
Therefore, our research question is as follows: Can a short virtual reality–based intervention applied preoperatively be effective in reducing patients’ anticipatory and treatment-related dental anxiety for those attending primary dental care? The aim is to apply short-term virtual reality relaxation (VRR) to examine if it is effective in reducing anticipatory and treatment-related dental anxiety in primary dental care through a randomized controlled trial (RCT) design.
Methods
Design
A randomized controlled single-center trial was conducted with 2 parallel arms: VRR and treatment as usual (TAU). Groups were randomized, following consent, with an allocation ratio of 1:1. No changes were made to methods after trial commencement.
Participants
Adult patients (≥18 y) who attended for dental treatment (basic, special, or emergency dental care; general anesthesia, x-ray), consented, and were able to complete the Finnish questionnaire without assistance were eligible for the study.
The study was conducted in the public Oral Health Care Unit of the Kalasatama Health and Welfare Center of the City of Helsinki, Finland. Patient recruitment and running the on-site research activities, such as administering the questionnaires and instructing the VRR group in the use of appliances, were conducted by 13 students from the Haaga-Helia University of Applied Sciences and Laurea University of Applied Sciences. Students were trained for this study by the lead clinician (S.L.) on-site to ensure uniformity of information provided to participants.
Patients were approached in 1 of the 2 arrival halls where they entered the Oral Health Care Unit. Patients were inquired if they had 15 min before their scheduled dental appointment to allow participation in the study. If the patients had the time and volunteered, they were told the nature of the study and given an information leaflet describing it and the possibility to win a movie ticket or xylitol products in a lottery after participation. If the patient consented, she or he was then randomized into 1 of the 2 groups.
Interventions
Interventions were conducted in similar settings in small alcoves with a seat and a table. The participants in the TAU group remained seated in the alcove for 3 min. Their experience of sitting in the alcove for 3 min was identical to that of the VRR group but without the VRR intervention. They were able to use their mobile phones if they so wished.
In the VRR group, participants chose 1 of the 5 videos (1 to 3.5 min). Still pictures of each video are provided in the Appendix. The application by MelloVR presented these videos. When the application was launched, clear instructions were displayed on the screen regarding next steps. These included basic instructions on how to select a video by turning one’s head toward a specific video via the so-called gaze selection method without manual controllers. The 360° videos (resolution range, 4,096 × 2,010 to 5,120 × 2,560) immersed the participants in a peaceful virtual landscape (beach, waterfall, underwater, space float, paddling). Videos were played with a Samsung Gear VR headset and a Samsung Galaxy S7 mobile phone (attached to the virtual headset) for the MelloVR application, with a total weight of approximately 500 g. A disposable mask was used with the headset for hygienic purposes.
Audio features and sound supported the relaxation experience. The musical ambient track was the same for all video choices. The file format is AAC with 320-kbps quality playing at 48 kHz. It has a tempo of 120 bpm (beats per minute) and fades in smoothly within 10 s. The musical instrumentation consists of a smooth synth pad, soft kick drum, and occasional bass and bell notes. White noise can be heard on top of the track, which listeners might find relaxing, particularly people with tinnitus. The synth pad looped the same harmony throughout the musical track, and the bass supports it. The bell instrument can be heard a few times, but no specific theme is recognized. This is typical of musical productions that are not meant to raise significant attention. The sound was played with on-ear headphones by Pioneer (model SE-M521) to exclude noise. The picture could be adjusted to suit the user’s eyesight by using the scroll on top of the glasses, and the audio volume could be set accordingly with a control on the side of the glasses.
Acceptability and feasibility of the VRR application were pilot tested prior to the RCT in 55 primary health care and social welfare clients of the Kalasatama Health and Welfare Center. Students who later recruited participants in the RCT invited volunteering clients to try a relaxing virtual reality experience. The virtual reality content and the devices were similar to those in the study. Volunteers’ perceptions were assessed after the virtual reality experience. Of the pilot participants, 98% found the experience relaxing; 87% would like to use it during a potentially anxiety-provoking treatment procedure; and 80% would recommend it to friends. Minor harmful effects, such as feelings of dizziness or nausea, were reported by <4%.
Outcomes
The main outcome measure, dental anxiety, was assessed with the validated Finnish version of the Modified Dental Anxiety Scale (MDAS) before and immediately after the intervention (Humphris et al. 2000; Yuan et al. 2008; Humphris et al. 2013). The measure has 5 questions, each with 5 reply alternatives from not anxious to extremely anxious. The primary outcome variable was the posttest MDAS total score. The secondary outcome variables were posttest scores for the 2 subscales of the MDAS: anticipatory dental anxiety (MDAS items 1 and 2) and treatment-related dental anxiety (MDAS items 3 to 5). After the intervention and completion of the posttest MDAS, patients reported their gender (female, male, other) and age in full years before attending their scheduled dental appointment. No personal information or information related to dental appointments after the study was collected.
From the MDAS, sums were calculated for the primary outcome total scale (range, 5 to 25) and for the secondary outcomes: anticipatory dental anxiety (range, 2 to 10) and treatment-related dental anxiety (range, 3 to 15).
Sample Size
Power calculation was estimated by the Stata “rsquared” routine. The effect of blocking was not introduced; however, the effect size was set to a low level to ensure a conservative approach when estimating a sufficient sample size. A small effect size of 0.04 in favor of the VRR intervention as compared with TAU would require a sample size of 272 participants at 90% power with alpha set to 0.05, 2-sided. This was calculated by specifying 2 control covariates (pretest MDAS and participant age in years) and the test random assignment factor (0 = TAU, 1 = VRR). Due to the chosen block size of 10 participants, the study required 280 participants.
Randomization
A random allocation sequence was computer generated by A.S. using random number lists in blocks of 10. The blocked randomization was used to keep the numbers of patients in both treatment groups closely balanced during the study and thus to homogenize the variation in group allocation due to patient flow in different weekdays and time of day. The block size of 10 was big enough to prevent guessing the next randomized treatment group, thus reducing bias (Altman 1991). The block size of 10 was also the multiple of number of treatments, and the required sample size was divisible by block size. The students enrolling the participants administered the randomization of patients, allocating the patient to the next free identification number on the randomization list. The patients were blinded until the intervention started. It was not possible to blind the students enrolling the patients.
Statistical Analyses
The primary outcome variable, posttest MDAS total score, was adjusted for the baseline (pretest) MDAS total score and participant age through mixed effects regression with inclusion of the random block effect. The analysis method ignoring blocks is more conservative regarding the statistical significance and thus less efficient and powerless (Matts and Lachin 1988). The analyses were repeated for the secondary outcome variables: MDAS anticipatory and treatment-related dental anxiety. Separate analyses were run for males and females. To avoid making assumptions of strict normality and nonheteroscedasticity, the “robust” option in the “regress” procedure was applied. Residual plots were inspected for identification of possible violations. Alpha was set to 0.05 (2-sided). Data were analyzed with Stata 15.1 (StataCorp 2017).
Ethics
Ethical approval was granted by the City of Helsinki (HEL 2018-008940). The trial was registered at ClinicalTrials.gov (NCT03993080).
Results
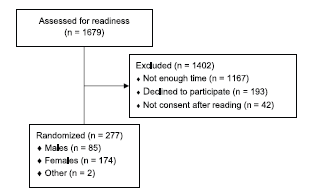
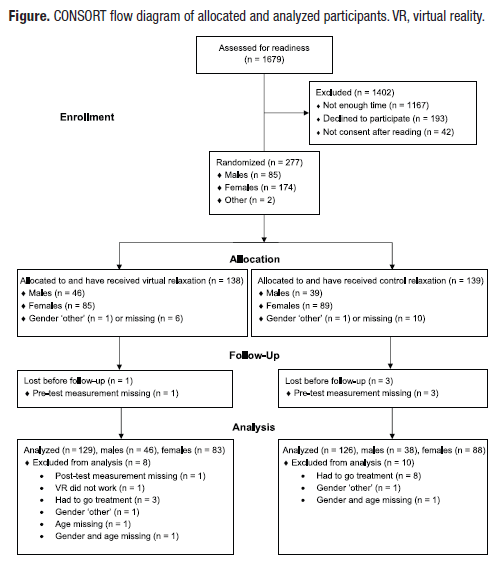
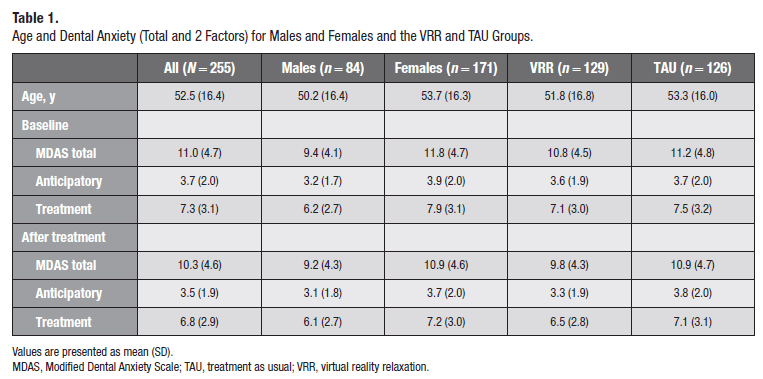
The flowchart of allocated and analyzed participants is presented in the Figure. Data collection started October 15, 2018, and was completed February 27, 2019. Recruitment was halted at 277 participants, who were analyzed by original assigned groups. Means and standard deviations for age and the MDAS total, anticipatory, and treatment-related anxiety scores according to gender and intervention group are presented in Table 1. Of the participants, 47.5% reported low dental anxiety (MDAS <10); 43.9%, moderate dental anxiety (MDAS, 10 to 18); and 8.6%, high dental anxiety (MDAS ≥19).
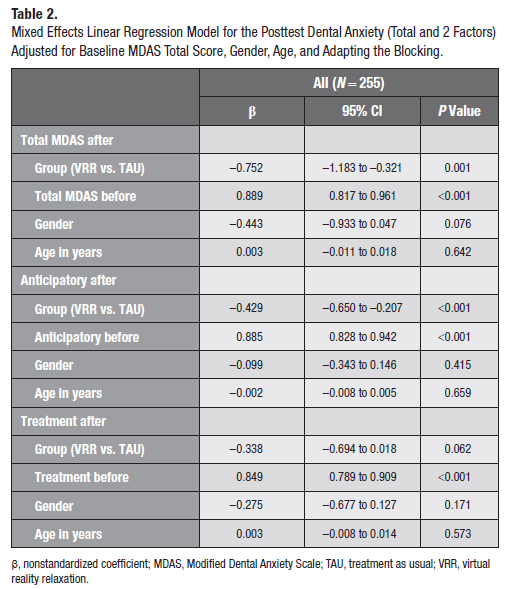
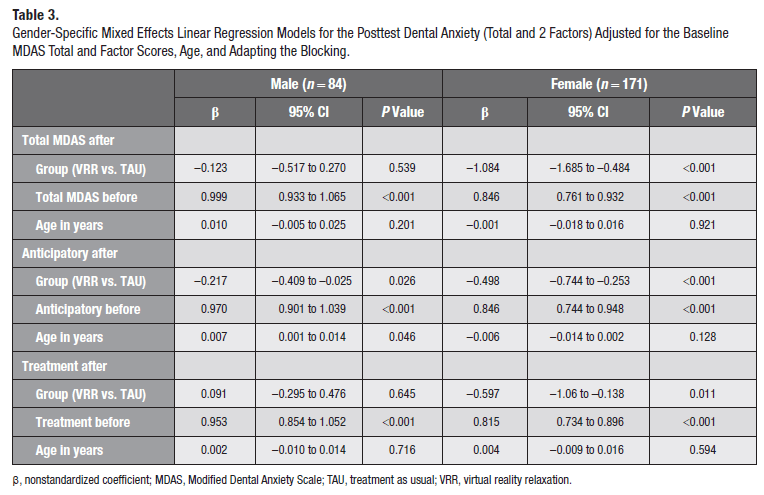
Group had a statistically significant effect in the total MDAS model and anticipatory dental anxiety model (Table 2). The VRR group showed 0.75–MDAS scale unit decrease in total dental anxiety and a 0.43–scale unit decrease in the anticipatory dental anxiety as compared with the TAU group. In the secondary gender-specific analyses, the females in the VRR group showed a >1–MDAS scale unit decrease in dental anxiety as compared with the TAU group. For males, the decrease was not statistically significant. In MDAS anticipatory dental anxiety. the VRR group showed a half–scale unit decrease as compared with the TAU group in females and a 0.2-unit decrease in males. For treatment-related dental anxiety, the decrease in MDAS scores was statistically significant only among females in the VRR group, showing over a half–scale unit decrease as compared with the TAU group (Table 3).
The MDAS outcome data showed a significant level of skewness. The “robust” option in Stata was applied to mitigate this. To check that our analyses were unbiased, we repeated the regression analyses with log-transformed dependent variable. All statistical results remained substantively the same.
Discussion
A short preoperative VRR decreased total and anticipatory dental anxiety in those attending a primary dental care clinic. In the secondary gender-specific analyses, total and treatment-related dental anxiety decreased among females and anticipatory dental anxiety among males. To our knowledge, this is the first study with a short VRR method in a routine dental primary care setting. Like Ganry et al. (2018), we found that even a short application of VRR reduced anticipatory dental anxiety.
It is possible that at least part of the dental anxiety reduction came from distraction, which has been shown to be effective when applied during dental treatment (Frere et al. 2001; Asl Aminabadi et al. 2012; Tanja-Dijkstra et al. 2014; Padrino-Barrios et al. 2015; Atzori et al. 2018; Niharika et al. 2018; Shetty et al. 2019). The virtual reality used in this study was developed for relaxation purposes. Regardless of the pathway, the use of virtual reality preoperatively reduced dental anxiety.
The strengths of this study are the RCT design and the study population, which included participants with all levels of dental anxiety in the primary dental care setting. The levels of dental anxiety were similar to the UK population norms (Humphris et al. 2013). We did not aim to maximize the effect of VRR by recruiting participants with high levels of dental anxiety only. Also, the intervention setup was very similar for both groups in terms of seating and the possibility for the TAU group to use a mobile phone, thus enabling the effect of the virtual reality intervention to be explicitly identified. The study did not assess dental anxiety levels after dental treatment or the type of treatment procedures that participants were receiving. Neither was the content or length of the VRR intervention that participants chose assessed, as this was a population study. Thus, the long-term effects and the effects of different VRR interventions as well as different dental treatments call for further studies.
There are also limitations to the study population. Recruiting took place in a setting with on average 200 patient visits per day. However, most patients arrived just in time for their scheduled appointment and did not have sufficient time to participate in the study (69.5% of those approached and 83.2% of those excluded). This might have led to possible bias in the age distribution, as older patients were more likely to arrive ahead of their scheduled appointments and thus participate the study. As another recruitment bias, we might have missed patients with high dental anxiety, as they may have come at the last minute. However, the percentages of participants with high dental anxiety were similar to the national survey among adult Finns (Liinavuori et al. 2016) and possibly due to the recruitment including patients coming for acute dental care. Only 11.5% of those approached declined to participate for other reasons, and 2.5% did not consent after reading the written information. The fact that many patients were unable to seek out VRR treatment due to time constraints needs to be addressed to ensure successful implementation at the population level.
There was also a lower percentage of men than women in this study, with only 3 men reporting high dental fear in this study. Men with high dental fear were underrepresented in another cohort study where dental anxiety was assessed in conjunction with dental examination (Kankaanpää et al. 2019). This might partly explain the lack of statistical significance of VRR among men and needs to be considered when powering future studies. Thus, results referring to the effect of gender should be interpreted with caution.
The positive findings of this study indicate that a short VRR intervention is a feasible, patient-accepted, inexpensive, and effective way of reducing preoperative dental anxiety in a public dental care setting on a population level. For those who are truly dentally phobic, we realize that more in-depth psychotherapeutic interventions are necessary. We therefore recommend in future studies that the level of dental anxiety be carefully inspected. In addition, further studies are needed to understand the effect of this VRR intervention more fully and to assess long-term outcomes.
Author Contributions
- Lahti, G. Humphris, contributed to conception, design, data analysis, and interpretation, drafted and critically revised the manuscript; A. Suominen, contributed to design, data analysis, and interpretation, drafted and critically revised the manuscript; R. Freeman, contributed to conception, design, and data interpretation, drafted and critically revised the manuscript; T. Lähteenoja, contributed to design and data interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Acknowledgements
The authors acknowledge MelloVR for providing the virtual reality relaxation equipment, the Oral Health Care Unit of Kalasatama Health and Welfare Center of the City of Helsinki for allowing access to their patients, and the students of the Haaga-Helia University of Applied Sciences and Laurea University of Applied Sciences for recruiting the participants.
Source
https://pmc.ncbi.nlm.nih.gov/articles/PMC6952244/
References
- Altman, DG . 1991. Practical statistics for medical research. Croydon (UK): CPI Group. p. 87–88.
- Armfield, JM . 2010. The extent and nature of dental fear and phobia in Australia. Aust Dent J. 55(4):368–377.
- Armfield, JM, Heaton, LJ. 2013. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 58(4):390–407.
- Asl Aminabadi, N, Erfanparast, L, Sohrabi, A, Ghertasi Oskouei, S, Naghili, A. 2012. The impact of virtual reality distraction on pain and anxiety during dental treatment in 4–6 year-old children: a randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospect. 6(4):117–124.
- Åstrøm, AN, Skaret, E, Haugejorden, O. 2011. Dental anxiety and dental attendance among 25-year-olds in Norway: time trends from 1997 to 2007. BMC Oral Health. 11:10.
- Atzori, B, Grotto, RL, Giugni, A, Calabrò, M, Alhalabi, W, Hoffman, HG. 2018. Virtual reality analgesia for pediatric dental patients. Front Psychol. 9:2265.
- Carlsson, V, Hakeberg, M, Wide Boman, U. 2015. Associations between dental anxiety, sense of coherence, oral health-related quality of life and health behavior—a national Swedish cross-sectional survey. BMC Oral Health. 15:100.
- Craske, MG, Treanor, M, Conway, CC, Zbozinek, T, Vervliet, B. 2014. Maximizing exposure therapy: an inhibitory learning approach. Behav Res Ther. 58:10–23.
- Frere, CL, Crout, R, Yorty, J, McNeil, DW. 2001. Effects of audiovisual distraction during dental prophylaxis. J Am Dent Assoc. 132(7):1031–1038.
- Ganry, L, Hersant, B, Sidahmed-Mezi, M, Dhonneur, G, Meningaud, JP. 2018. Using virtual reality to control preoperative anxiety in ambulatory surgery patients: a pilot study in maxillofacial and plastic surgery. J Stomatol Oral Maxillofac Surg. 119(4):257–261.
- Gordon, D, Heimberg, RG, Tellez, M, Ismail, AI. 2013. A critical review of approaches to the treatment of dental anxiety in adults.J Anxiety Disord. 27(4):365–378.
- Gujjar, KR, van Wijk, A, Kumar, R, de Jongh, A. 2019a. Are technology-based interventions effective in reducing dental anxiety in children and adults? A systematic review. J Evid Based Dent Pract. 19(2):140–155.
- Gujjar, KR, van Wijk, A, Kumar, R, de Jongh, A. 2019b. Efficacy of virtual reality exposure therapy for the treatment of dental phobia in adults: a randomized controlled trial.J Anxiety Disord. 62:100–108.
- Gujjar, KR, van Wijk, A, Sharma, R, de Jongh, A. 2017. Virtual reality exposure therapy for the treatment of dental phobia: a controlled feasibility study. Behav Cogn Psychother. 46(3):367–373.
- Hägglin, C, Berggren, U, Hakeberg, M, Hallstrom, T, Bengtsson, C. 1999. Variations in dental anxiety among middle-aged and elderly women in Sweden: a longitudinal study between 1968 and 1996. J Dent Res. 78(10):1655–1661.
- Hakeberg, M, Wide Boman, U. 2017. Dental care attendance and refrainment from dental care among adults. Acta Odontol Scand. 75(5):366–371.
- Hill, KB, Chadwick, B, Freeman, R, O’Sullivan, I, Murray, JJ. 2013. Adult Dental Health Survey 2009: relationships between dental attendance patterns, oral health behaviour and the current barriers to dental care. Br Dent J. 214(1):25–32.
- Humphris, GM, Crawford, JR, Hill, K, Gilbert, A, Freeman, R. 2013. UK population norms for the modified dental anxiety scale with percentile calculator: adult dental health survey 2009 results. BMC Oral Health. 13:29.
- Humphris, GM, Freeman, R, Campell, J, Tuutti, H, D’Souza, V. 2000. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 50(6): 367–370.
- Kankaanpää, R, Auvinen, J, Rantavuori, K, Jokelainen, J, Karppinen, J, Lahti, S. 2019. Pressure pain sensitivity is associated with dental fear in adults in middle age: findings from the Northern Finland 1966 birth cohort study. Community Dent Oral Epidemiol. 47(3):193–200.
- Kazancioglu, HO, Tek, M, Ezirganli, S, Demirtas, N. 2015. Does watching a video on third molar surgery increase patients’ anxiety level? Oral Surg Oral Med Oral Pathol Oral Radiol. 119(3):272–277.
- Lahti, S, Vehkalahti, MM, Nordblad, A, Hausen, H. 2007. Dental fear among population aged 30 years and older in Finland. Acta Odontol Scand. 65(2):97–102.
- Liinavuori, A, Tolvanen, M, Pohjola, V, Lahti, S. 2016. Changes in dental fear among Finnish adults: a national survey. Community Dent Oral Epidemiol. 44(2):128–134.
- Liinavuori, A, Tolvanen, M, Pohjola, V, Lahti, S. 2019. Longitudinal interrelationships between dental fear and dental attendance among adult Finns in 2000–2011. Community Dent Oral Epidemiol. 47(4):309–315.
- Maggirias, J, Locker, D. 2002. Five-year incidence of dental anxiety in an adult population. Community Dent Health. 19(3):173–179.
- Matts, JP, Lachin, JM. 1988. Properties of permuted-block randomization in clinical trials. Controlled Clinical Trials. 9(4):327–344.
- Niharika, P, Reddy, NV, Srujana, P, Srikanth, K, Daneswari, V, Geetha, KS. 2018. Effects of distraction using virtual reality technology on pain perception and anxiety levels in children during pulp therapy of primary molars. J Indian Soc Pedod Prev Dent. 36(4):364–369.
- Padrino-Barrios, C, McCombs, G, Diawara, N, De Leo, G. 2015. The use of immersive visualization for the control of dental anxiety during oral debridement. J Dent Hyg. 89(6):372–377.
- Pohjola, V, Lahti, S, Vehkalahti, MM, Tolvanen, M, Hausen, H. 2007. Association between dental fear and dental attendance among adults in Finland. Acta Odontol Scand. 65(4):224–230.
- Google Scholar | Crossref | Medline
- Raghav, K, Van Wijk, AJ, Abdullah, F, Islam, MN, Bernatchez, M, De Jongh, A. 2016. Efficacy of virtual reality exposure therapy for treatment of dental phobia: a randomized control trial. BMC Oral Health. 16:25.
- Rooksby, M, Elouafkaoui, P, Humphris, G, Clarkson, J, Freeman, R. 2015. Internet-assisted delivery of cognitive behavioural therapy (CBT) for childhood anxiety: systematic review and meta-analysis. J Anxiety Disord. 9:83–92.
- Shetty, V, Suresh, LR, Hegde, AM. 2019. Effect of virtual reality distraction on pain and anxiety during dental treatment in 5–8-year-old children. J Clin Pediatr Dent. 43(2):97–102.
- StataCorp . 2017. Stata Statistical Software: Release 15. College Station (TX): StataCorp LLC.
- Tanja-Dijkstra, K, Pahl, S, White, MP, Andrade, J, Qian, C, Bruce, M, May, J, Moles, DR. 2014. Improving dental experiences by using virtual reality distraction: a simulation study. PLoS One. 9(3):e91276.
- Tellez, M, Potter, CM, Kinner, DG, Jensen, D, Waldron, E, Heimberg, RG, Myers Virtue, S, Zhao, H, Ismail, AI. 2015. Computerized tool to manage dental anxiety: a randomized clinical trial. J Dent Res. 94(9):174S–180S.
- Thomson, WM, Broadbent, JM, Locker, D, Poulton, R. 2009. Trajectories of dental anxiety in a birth cohort. Community Dent Oral Epidemiol. 37(3):209–219.
- Thomson, WM, Williams, SM, Broadbent, JM, Poulton, R, Locker, D. 2010. Long-term dental visiting patterns and adult oral health. J Dent Res. 89(3):307–311.
- Wide Boman, U, Carlsson, V, Westin, M, Hakeberg, M. 2013. Psychological treatment of dental anxiety among adults: a systematic review. Eur J Oral Sci. 121(3, pt 2):225–234.
- Yuan, S, Freeman, R, Lahti, S, Lloyd-Williams, F, Humphris, G. 2008. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual Life Outcomes. 6:22.