
Augmented Reality Innovation in Prosthodontics and Smile Design
ABSTRACT Prosthetic dentistry is one of the dental branches that has evolved remarkably, taking advantage of the latest digital innovations. […]

ABSTRACT Prosthetic dentistry is one of the dental branches that has evolved remarkably, taking advantage of the latest digital innovations. […]
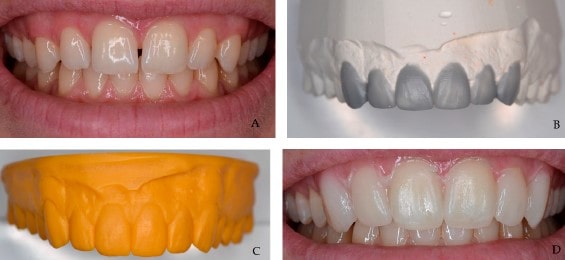
ABSTRACT Abstract: Introduction: Several methods are currently available for providing a preview of the prosthodontic treatment, including computer simulations, 3D
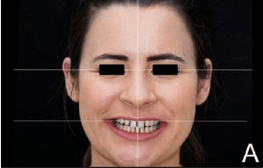
ABSTRACT The primary aim of aesthetic dental procedures is to meet patients’ expectations by enhancing facial and smile aesthetics. Over
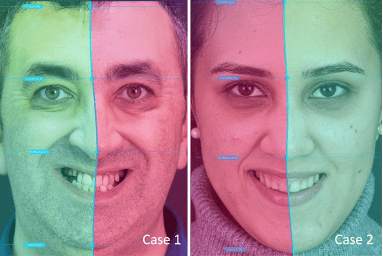
ABSTRACT This study evaluates the preference rates for smile designs created by professionals or by Artificial Intelligence (AI) among dentists,
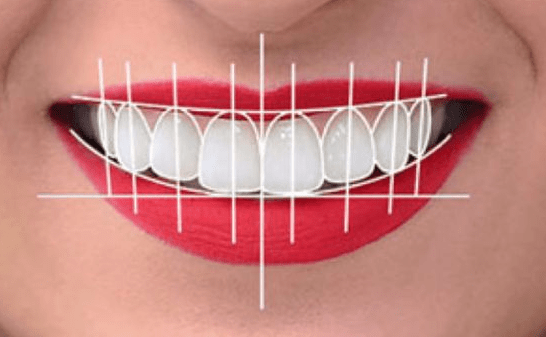
ABSTRACT Background: The esthetics of a smile holds significant importance in an individual’s self-esteem and overall quality of life. In
ABSTRACT Function Breakthroughs in technology have not been possible without influencing the medical sciences. Dentistry and dental materials have been
ABSTRACT Abstract: One of the important ways of social interaction is through verbal and nonverbal communication. The human face is
ABSTRACT Abstract: Background: Augmented reality (AR) enhances sensory perception by adding extra information, improving anatomical localization and simplifying treatment views.
ABSTRACT Fine motor skill is indispensable for a dentist. As in many other medical fields of study, the traditional surgical
ABSTRACT Abstract : The OSCE is a reliable evaluation method to estimate the preclinical examination of dental students. The most